Transforming Rare Disease Care Through AI — Design Thinking Workshop at UC Berkeley
The rare disease journey can feel like navigating an uncertain space where past health experiences recede and the present is defined by what one panelist called "obscuropathy" — a presentation of symptoms without a clear cause. Patients experience years without an answer. Symptoms are dismissed or misattributed during brief medical encounters. The burden of getting to a diagnosis falls on them and their families. As the experts put it: "Institutional infrastructure keeps us disconnected," creating gulfs between doctors, patients, and researchers that no individual clinician can bridge alone.
On April 19, 2025, we convened an AI Innovation Challenge at UC Berkeley — co-organized with Berkeley AMENA, Berkeley Haas Entrepreneurship, the UC Berkeley Blum Center, INSE Corps, and NSF Innovation Corps — to explore what AI-driven, human-centered design could actually do for this community. Not in the abstract. In six hours, with real teams, building real prototypes.
The talks
Dr. Mohsen Hejrati opened with the AI landscape — specifically what becomes possible when models can read, listen, see, and suggest instantly across the fragmented data rare disease patients accumulate over years. He grounded it in concrete cases: an AI co-scientist that resolved a long-standing research problem in two days; a mother who used ChatGPT to identify her son's rare spinal condition after multiple physicians had not. Beyond text, AI can now detect rare genetic conditions from facial features or MRIs, sometimes performing comparably to clinicians. It can accelerate drug repurposing by analyzing datasets for new applications of existing molecules. For patients, it can answer condition-specific questions at 2am, translate complex science into plain language, and synthesize hundreds of papers to surface research gaps. The rapid expansion of medical knowledge has outpaced human capacity to hold it — AI is not replacing clinical judgment, it is making clinical judgment possible at scale.
Dr. Laurel Crosby Delof from Stanford's Genome Technology Center introduced a reframe that shifted the entire conversation: *Obscuropathy*. Not "rare disease" — a label that implies inherent unknowability — but a condition where there is an answer; we just don't know what it is yet. The diagnostic odyssey averages five years and seven-plus physicians. The barriers are structural: limited provider familiarity, reactive systems that require extreme illness severity before ordering genetic testing, institutional silos that keep the people who could solve the case from talking to each other. Her proposed model: solve one case, validate the pattern, share it — a "GitHub for medicine" where diagnostic logic is open, buildable-upon, and not siloed inside any single institution.
My session focused on the design thinking methodology for the afternoon's challenge, and on a tool I built for it: RareMap — an AI platform for exploring rare disease challenges through stakeholder mapping, pain point identification, and opportunity framing. The session also addressed what I think is the question most AI-for-health conversations skip: what does trust look like when the person you're designing for has already been failed, repeatedly, by systems that claimed to help them? Empathy + Insights = Impact is not a slogan. It is the correct sequencing. You build the empathetic foundation first — through deep listening, a clear Point of View, a specific "How Might We" — before you let AI generate anything.
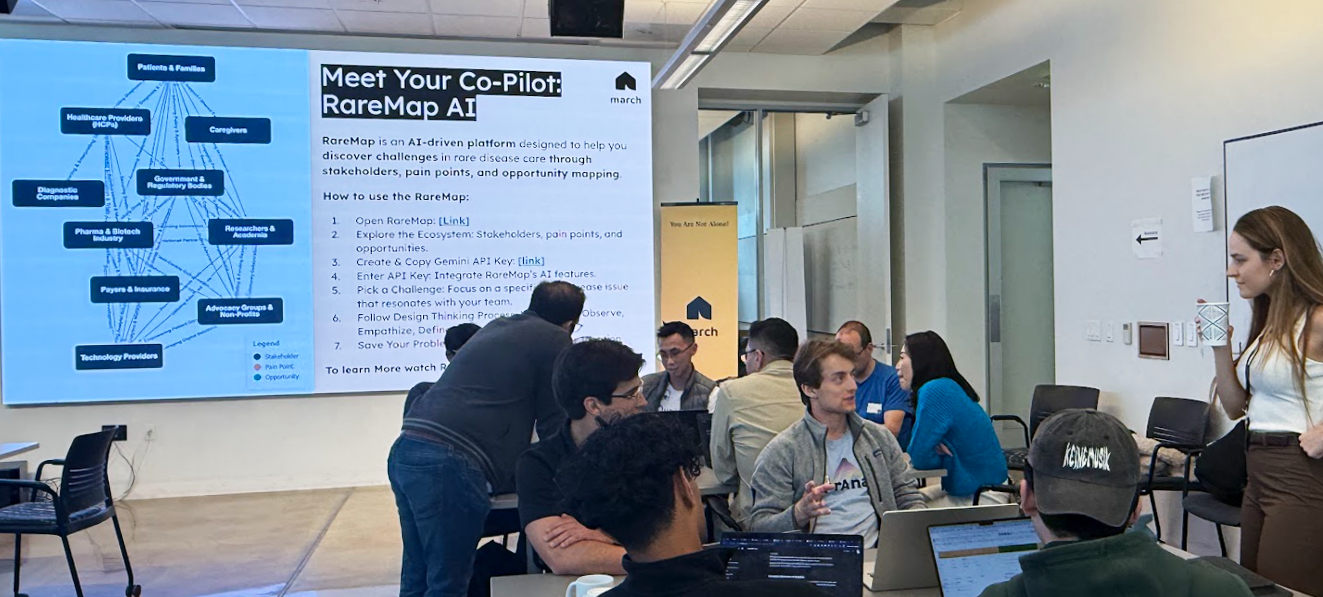
RareMap AI — stakeholder and opportunity mapping platform
The design thinking process
Teams moved through six stages: Empathize, Define, Ideate, Prototype, Test, Reflect. RareMap supported the Empathize and Define phases — teams used it to map the rare disease ecosystem, identify unmet needs, and select a specific challenge to address before moving into ideation.
In the Ideate phase, AI helped uncover patterns in sparse rare disease data and generate "what-if" scenarios. The emphasis remained on human oversight throughout: rare disease solutions require ethical alignment, especially given patient vulnerability and small datasets. AI generated options; empathy determined which ones actually served people.
Four considerations were non-negotiable across all teams:
Data Bias & Representation — rare disease datasets are small and historically non-diverse. Equitable outcomes require equitable training data.
Transparency & Explainability — clinicians and patients need accessible rationales, not black-box outputs. In a context where trust is already depleted, opaque models are not a design flaw; they are a disqualifying condition.
Regulatory & Ethical Constraints — HIPAA/GDPR compliance, informed consent, clear liability. Not bureaucratic hurdles — minimum conditions for operating responsibly with a vulnerable population.
Human-in-the-Loop — clinicians, domain experts, and patient advocates are the final decision-makers. The AI is the operator. The human is the director and reviewer.
Six prototypes
| Team | Problem | Solution | Technology |
|---|---|---|---|
| Stitch | Fragmented records, diagnostic delays, isolation | Secure AI health data vault — unified records, pattern matching, specialist and trial matching, peer connection | LLMs, Intelligent Querying |
| Quantoflow | Low clinical trial participation, patient unawareness, CRO recruitment inefficiency | Voice-based AI chatbot for early patient screening and guidance into clinical trials | Conversational AI, LLMs |
| Born | Caregiver overwhelm, emotional support needs, difficulty finding treatment options and peers | AI Brain Tumor Network Visualization and chatbot connecting caregivers to similar patients and treatment centers | Graph AI, LLM |
| Claim Clear | Physician burden from insurance documentation, delayed patient access | AI agent converting physician notes and EMR into reimbursement-ready evidence and CPT codes | LLM, Natural Language Processing |
| RareFind AI | Lack of high-quality standardized rare disease data for research and patient identification | Platform to retrieve, standardize, and provide multilingual real-world data across diverse sources | Named Entity Recognition, Multilingual Models |
| LEGS | Lost non-profit information, cumbersome traditional data collection | Gamified AI experience for high-quality data collection; long-term AI chatbot for institutional knowledge | Gamification AI, Intelligent Data Collection |
The range of problems addressed — fragmented records, clinical trial access, caregiver support, physician administrative burden, data standardization, institutional knowledge loss — collectively point at one thing: the system was not designed around the person with the most at stake. Every team found a different seam in the same structural failure. Without clean, integrated, accessible data, even the most empathetically designed application cannot function. Stitch and RareFind AI addressed the backbone. Quantoflow and Born addressed the human moments that fall through clinical cracks. Claim Clear addressed the inefficiency that directly delays access. LEGS addressed the knowledge that disappears when no one builds infrastructure to hold it.
During the panel discussion, an audience member shared their multi-million-dollar medical journey and their ongoing struggle to navigate solutions independently. JC Muyl, founder of MyRareData, took that moment and named it: patients have become their own vectors for finding answers. AI now gives those patients something they didn't have before — knowledge access, data synthesis, and communication tools that can turn a solo investigation into something that actually moves.
When asked about prevention versus treatment and individual health trends, Dr. Crosby's answer was consistent: "Show me the data." Generic advice fails individuals. Understanding specific biology — genetics, exposures, unique circumstances — is what makes personalized solutions possible. The diagnostic model she envisions is systematic: solve one case, validate it, share it. "If you solve the case and I solve a case and we all solve a case, we're going to get through all 10,000 of these rare diseases." Each solved case becomes a recognizable pattern the community can build on.
Dr. Ashtari drew a clear line between what AI handles well and what it does not. Informational needs, research synthesis, clarifying complex concepts — AI is genuinely useful there. But the emotional support and sense of belonging patients need extends beyond algorithmic solutions. It requires authentic human connection, potentially structured or facilitated by AI, but not replaced by it. That distinction — between what AI can accelerate and what it cannot substitute — shaped every design decision teams made during the prototyping phase, and is the most important thing I brought back from the room.
The workshop started with one structural claim — that obscuropathy is a solvable problem — and ended with six prototypes that proved the point from six different angles. Every team found fragmentation. Every team built something to reduce it. The data is too scattered. The care pathway is too disconnected. The patient is carrying too much alone. None of these are technical problems without solutions; they are prioritization problems without champions.
What the talks, the prototyping, and the panel discussion together made clear: the capability exists to build systems that genuinely serve this population. AI can synthesize what no individual clinician can hold. Design thinking can shape those systems around the people who actually need to trust them. And community — the kind Dr. Crosby imagines as a shared diagnostic commons, the kind Dr. Ashtari insists cannot be automated away — is what makes both of those things matter. The question the day left open is not whether it is possible. It is who decides it is worth doing.

Workshop at UC Berkeley

Teams working

Teams collaborating
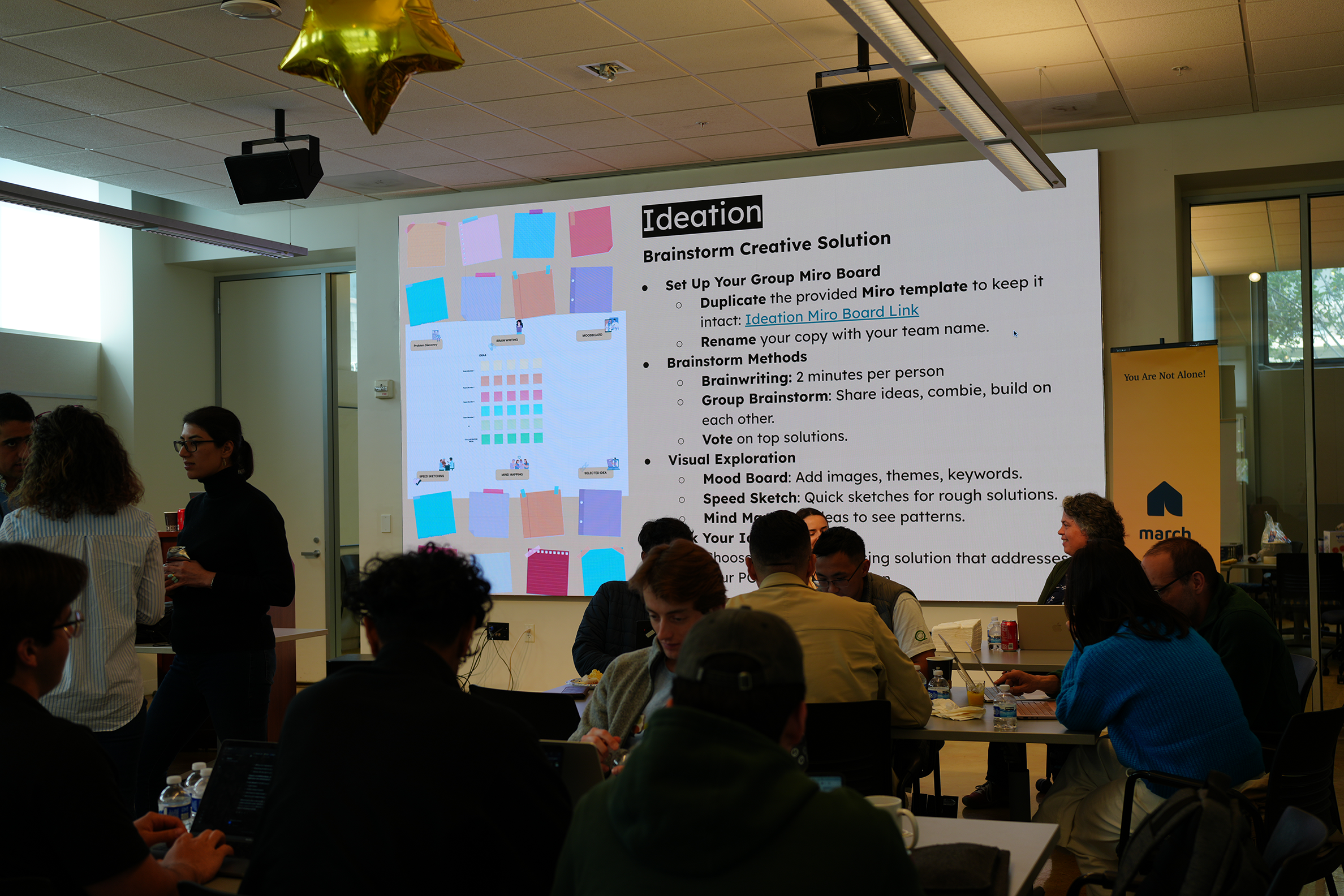
Ideation session
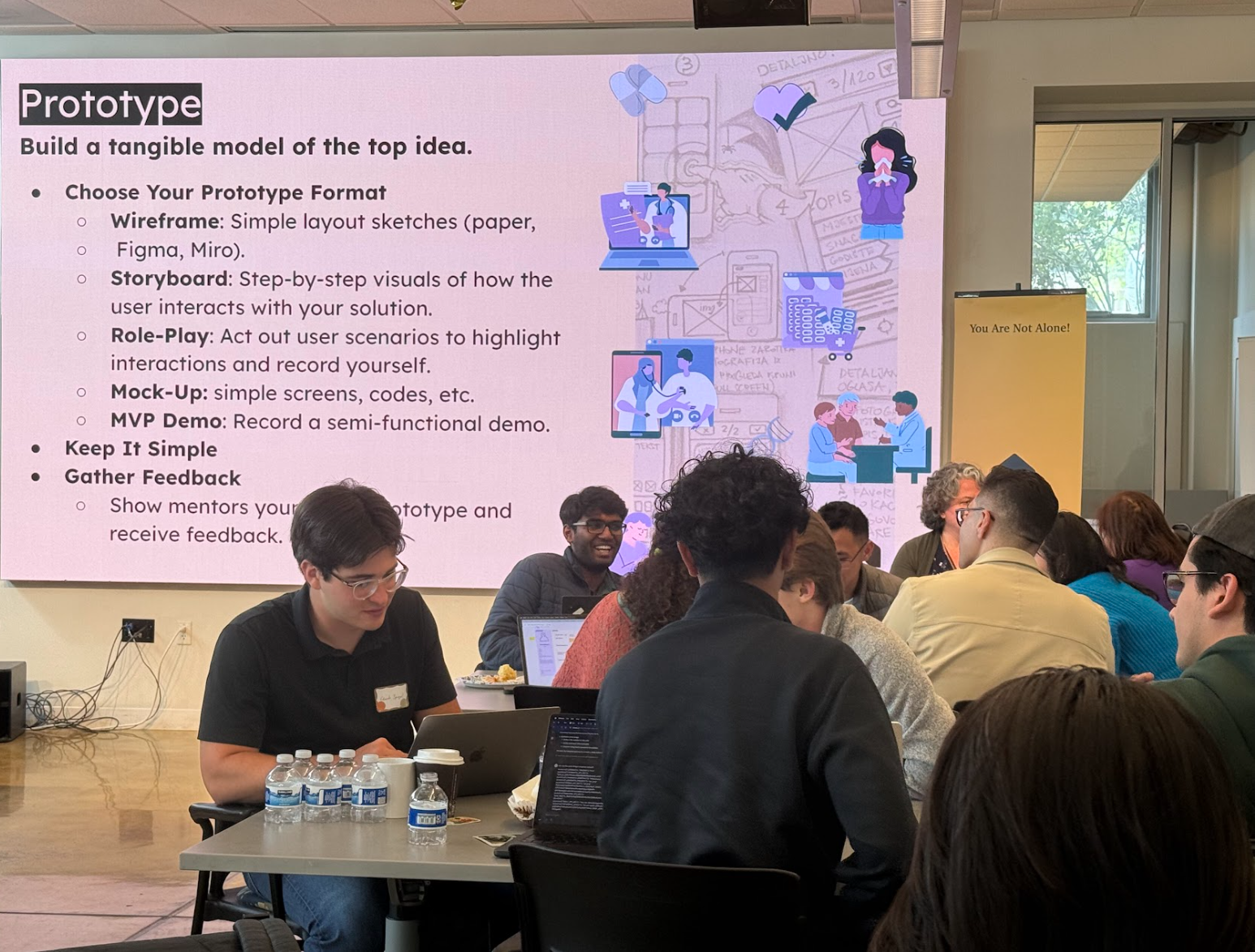
Prototyping phase